SimonMacMichael.jpg.43c0ea0f7feb7cf18b460c43173eeaec.jpg)

OLYMPIC
-
Posts
601 -
Joined
-
Last visited
-
Days Won
31
Posts posted by OLYMPIC
-
-
Understanding IGF-1
By Bryan Haycock
To understand how IGF-1 works you have to understand how muscles grow. The ability of muscle tissue to constantly regenerate in response to activity makes it unique. It’s ability to respond to physical/mechanical stimuli depends greatly on what are called satellite cells. Satellite cells are muscle precursor cells. You might think of them as "pro-muscle" cells. They are cells that reside on and around muscle cells. These cells sit dormant until called upon by growth factors such as IGF-1. Once this happens these cells divide and genetically change into cells that have nuclei identical to those of muscle cells. These new satellite cells with muscle nuclei are critical if not mandatory to muscle growth.
Without the ability to increase the number of nuclei, a muscle cell will not grow larger and its ability to repair itself is limited. The explanation for this is quite simple. The nucleus of the cell is where all of the blue prints for new muscle come from. The larger the muscle, the more nuclei you need to maintain it. In fact there is a "nuclear to volume" ratio that cannot be overridden. Whenever a muscle grows in response to functional overload there is a positive correlation between the increase in the number of myonuclei and the increase in fiber cross sectional area (CSA). When satellite cells are prohibited from donating new nuclei, overloaded muscle will not grow (Rosenblatt,1992 & 1994; Phelan,1997). So you see, one important key to unnatural muscle growth is the activation of satellite cells by growth factors such as IGF-1.
IGF-1 stimulates both proliferation (an increase in cell number) and differentiation (a conversion to muscle specific nuclei) in an autocrine-paracrine manner, although it induces differentiation to a much greater degree. This is in agreement with the Dual Effector theory. In fact, you can inject a muscle with IGF-1 and it will grow! Studies have shown that , when injected locally, IGF-1 increases satellite cell activity, muscle DNA content, muscle protein content, muscle weight and muscle cross sectional area (Adams,1998).
On the very cutting edge of research scientists are now discovering the signaling pathway by which mechanical stimulation and IGF-1 activity leads to all of the above changes in satellite cells, muscle DNA content, muscle protein content, muscle weight and muscle cross sectional area just outlined above. This research is stemming from studies done to explain cardiac hypertrophy. It involves a muscle enzyme called calcineurin which is a phosphatase enzyme activated by high intracellular calcium ion concentrations (Dunn, 1999). Note that overloaded muscle is characterized by chronically elevated intracellular calcium ion concentrations. Other recent research has demonstrated that IGF-1 increases intracellular calcium ion concentrations leading to the activation of the signaling pathway, and subsequent muscle fiber hypertrophy (Semsarian, 1999; Musaro, 1999). I am by no means a geneticist so I hesitated even bringing this new research up. In summary the researchers involved in these studies have explained it this way, IGF-1 as well as activated calcineurin, induces expression of the transcription factor GATA-2, which accumulates in a subset of myocyte nuclei, where it associates with calcineurin and a specific dephosphorylated isoform of the transcription factor nuclear factor of activated T cells or NF-ATc1. Thus, IGF-1 induces calcineurin-mediated signaling and activation of GATA-2, a marker of skeletal muscle hypertrophy, which cooperates with selected NF-ATc isoforms to activate gene expression programs leading to increased contractile protein synthesis and muscle hypertrophy. Did you get all that?
IGF-1 Usage
By Author Unkown
IGF stands for insulin-like growth factor. It is a natural substance that is produced in the human body and is at its highest natural levels during puberty. During puberty IGF is the most responsible for the natural muscle growth that occurs during these few years. There are many different things that IGF does in the human body; I will only mention the points that would be important for physical enhancement. Among the effects the most positive are increased amino acid transport to cells, increased glucose transport, increased protein synthesis, decreased protein degradation, and increased RNA synthesis.
When IGF is active it behaves differently in different types of tissues. In muscle cells proteins and associated cell components are stimulated. Protein synthesis is increased along with amino acid absorption. As a source of energy, IGF mobilizes fat for use as energy in adipose tissue. In lean tissue,
IGF prevents insulin from transporting glucose across cell membranes. As a result the cells have to switch to burning off fat as a source of energy.
IGF also mimic's insulin in the human body. It makes muscles more sensitive to insulin's effects, so if you are a person that currently uses insulin you can lower your dosage by a decent margin to achieve the same effects, and as mentioned IGF will keep the insulin from making you fat.
Perhaps the most interesting and potent effect IGF has on the human body is its ability to cause hyperplasia, which is an actual splitting of cells. Hypertrophy is what occurs during weight training and steroid use, it is simply an increase in the size of muscle cells. See, after puberty you have a set number of muscle cells, and all you are able to do is increase the size of these muscle cells, you don't actually gain more. But, with IGF use you are able to cause this hyperplasia which actually increases the number of muscle cells present in the tissue, and through weight training and steroid usage you are able to mature these new cells, in other words make them grow and become stronger. So in a way IGF can actually change your genetic capabilities in terms of muscle tissue and cell count. IGF proliferates and differentiates the number of types of cells present. At a genetic level it has the potential to alter an individuals capacity to build superior muscle density and size.
There is a lot of talk about the similarity between IGF and growth hormone. The most often asked question is simply which is more effective. GH doesn't directly cause your muscles to grow, it works very indirectly by increasing protein synthesis capabilities, increasing the amount of insulin a person can use effectively, and increasing the amount of anabolic steroids a person can use effectively. GH also indirectly causes muscle growth by stimulating the release of IGF when it (the GH) is destroyed in the human body. So one way you could look at it as GH being a precursor to IGF. So to put it simple IGF is more effective at directly causing muscle growth and density increases. IGF is also much more cost effective.
IGF can also be effectively used by itself and gains will still be easily noticeable. With growth hormone you need to use high amounts of anabolics and often insulin to see any gains at all, this is not the case with IGF. IGF can be used by itself and is often used by bodybuilders who bridge between cycles, during this bridge is a good time to use IGF since it has no effect on natural testosterone production so it will therefore allow you to return to normal in terms of hormone levels. A stack of IGF, PGF2a, HCG, and clomid would be a good bridge stack and would allow your body to return to normal and still allow you to retain and make new gains.
IGF is a research drug, it hasn't been approved by the FDA for use as a pharmaceutical and it is currently being researched for nerve tissue repair, possible burn victims, and also as a possible aid in muscle wasting for AIDS patients. There are many different analogs of IGF available, instead of mentioning them all, I will simply mention the two most common and the most effective. Regular recombinant IGF is one of the two, it is also the more expensive and the least effective. Regular IGF only has a half-life of about 10-20 minutes in the human body and is quickly destroyed, it can be combined with certain binding proteins to extend the half-life, but it is not a very simple procedure and there is a more effective and less expensive version available. The most effective form of IGF is Long R3 IGF-1, it has been chemically altered and has had amino acid changes which cause it to avoid binding to proteins in the human body and allow it to have a much longer half life, around 20-30 hours. "Long R3 IGF-1 is an 83 amino acid analog of IGF-1 comprising the complete human IGF-1 sequence with the substition of an Arg(R) for the Glu(E) at position three, hence R3, and a 13 amino acid extension peptide at the N terminus. This analog of IGF-1 has been produced with the purpose of increasing the biological activity of the IGF peptide."
"Long R3 IGF-1 is signifacantly more potent than IGF-1. The enhanced potency is due to the decreased binding of Long R3 IGF-1 to all known IGF binding proteins. These binding proteins normally inhibit the biological actions of IGF's."
It is also not as expensive since a media grade version is available which is sufficient for bodybuilding use. There is also a receptor grade available but it is VERY expensive and the only noticeable difference between the two would only be able to be noticed in a laboratory setting. The price on the black market for Long R3 IGF-1 can be seen anywhere from $200-$500 per milligram depending on the source.
The most effective length for a cycle of IGF is 50 days on and 20-40 days off. The most controversy surrounding Long R3 IGF-1 is the effective dosage. The most used dosages range between 20mcg/day to 120+mcg/day. IGF is only available by the milligram, one mg will give you a 50 day cycle at 20mcg/day, 2mg will give you a 50 day cycle at 40mcg/day, 3mg will give you a 50 day cycle at 60mcg/day, 4mg will give you a 50 day cycle at 80mcg/day and so on. The dosage issue mainly revolves around how much money you have to spend, plenty of people use the minimum dosage of 20mcg/day and are happy with the results, and in fact several top bodybuilders use the 20mcg/day dosage and are pleased with the results. IGF is most effective when administered subcutaneously and injected once or twice daily at your current dosage. The best time for injections is either in the morning and/or immediately after weight training.
Another frequently asked question of IGF refers to the real world results, in terms of pure weight gain don't expect to gain 5 lbs. a week like you may off of anadrol or a similar steroid. The only weight you will gain from IGF use is pure lean muscle tissue, with steroids most of the weight gained is water weight. With an effective dosage you can expect to gain 1-2 lbs of new lean muscle tissue every 2-3 weeks and these effects can be increased with the use of testosterone, anabolic steroids, and insulin use. Increased vascularity is also very common, people report seeing veins appear where they never have before. And yet another effect reported is the ability to stay lean while bulking with heavy dosages of steroids and TONS of food while on an IGF cycle, this is perhaps the most pleasing effect. Increased pumps are also noticeable almost immediately, the pumps can almost become painful, pumps are even noticeable when doing cardio.
Overall, IGF is a very exciting drug due to its ability to alter ones genetic capabilities. If you can find a trustworthy source and you use it correctly it can be a VERY useful tool in your bodybuilding drug arsenal.
-
 3
3
-
-
Enjoy the read Northerners
Proviron is a synthetic, orally effective androgen which does not have any anabolic characteristics. Proviron is used in school medicine to ease or cure disturbances caused by a deficiency of male sex hormones. Many athletes, for this reason, often use Proviron at the end of a steroid treatment in order to increase the reduced testosterone production. This, however is not a good idea since Proviron has no effect on the body's own testosterone production but-as mentioned in the beginning-only reduces or completely eliminates the dysfunctions caused by the testosterone deficiency. These are in particular impotence which is mostly caused by an androgen deficiency that can occur after the discontinuance of steroids, and infertility which manifests itself in a reduced sperm count and a reduced sperm quality. Proviron is therefore taken during a steroid administration or after discontinuing the use of the steroids, to eliminate a possible impotency or a reduced sexual interest. This, however does not contribute to the maintainance of strength and muscle mass after the treatment. There are other better suited compounds for this (see HCG and Clomid). For this reason Proviron is unfortunately cunsidered by many to be a useless and unnecessary compound.
You should be aware that Proviron is also an estrogen antagonist which prevents the aromatization of steroids. Unlike the antiestrogen Nolvadex which only blocks the estrogen receptors (see Nolvadex) Proviron already prevents the aromatizing of steroids. Therefore gynecomastia and increased water retention are successfully blocked. Since Proviron strongly suppresses the forming of estrogens no rebound effect occurs after discontinuation of use of the compound as is the case with, for example, Nolvadex where an aromatization of the steroids is not prevented. One can say that Nolvadex cures the problem of aromatization at its root while Nolvadex simply cures the symptoms. For this reason male athletes should prefer Proviron to Nolvadex. With Proviron the athlete obtains more muscle hardness since the androgen level is increased and the estrogen concentration remains low. This, in particular, is noted positively during the preparation for a competition when used in combination with a diet. Female athletes who naturally have a higher estrogen level often supplement their steroid intake with Proviron resulting in an increased muscle hardness. In the past it was common for bodybuilders to take a daily dose of one 25 mg tablet over several weeks, sometimes even months, in order to appear hard all year round. This was especially important for athletes appearances at guest performances, seminars and photo sessions. Today Clenbuterol is usually taken over the entire year since possible virilization symptoms cannot occur which is not yet the case with Proviron. Since Proviron is very effective male athletes usually need only 50 mg/day which means that the athlete usually takes one 25 mg tablet in the morning and another 25 mg tablet in the evening. In some cases one 25 mg tablet per day is sufficient. When combining Proviron with Nolvadex (50 mg Proviron/day and 20 mg Nolvadex/day) this will lead to an almost complete suppression of estrogen.
The side effects of Proviron in men are low at a dosage of 2-3 tablets/day so that Proviron, taken for example in combination with a steroid cycle, can be used comparatively without risk over several weeks. Since Proviron is well-tolerated by the liver liver dysfunctions do not occur in the given dosages. For athletes who are used to acting under the motto "more is better" the intake of Proviron could have a paradoxical effect. The most common side effect of Proviron-or in this case, secondary symptom- is in part a distinct sexual overstimulation and in some cases continuous penis erection. Since this condition can be painful and lead to possible damages, a lower dosage or discontinuing the compound are the only sensible solutions. Female athletes should use Proviron with caution since possible androgenic side effects cannot be excluded. Women who want to give Proviron a try should not take more than one 25 mg tablet per day. Higher dosages and periods of intake of more than four weeks considerably increase the risk of virilization symptoms. Female athletes who have no difficulties with Proviron obtain good results with 25 mg Proviron/day and 20 mg Nolvadex/day and, in combination with a diet, report an accelerated fat breakdown and continuously harder muscles.
-
1
-
-
It is so important not to chronically elevate GH and especially IGF-1. What follows is a summation of GH, how it acts, where it acts and its involvement in disease states.
Derived in part from patent filings of GH-receptor antagonists.
What is it?
Growth hormone (GH) is in its major form, a 22-kDa (22 kilodalton) protein consisting of 191 amino acids (in humans), and in its equally anabolic minority isoform, a 20-kDa protein consisting of the same structure with the deletion of 15 amino acids at positions 32 to 46 as well as dimers of these two forms, released by the pituitary and a member of a cascade of hormones that regulate the growth of the body and its organs. Various Fragments of the GH chain are also released and may undergo further cleavage into yet other fragments. The biological activity for most of the fragments are known yet their significance and "modes of action" remain to be elucidated.
Secretion of growth hormone into the bloodstream is followed by binding to growth hormone receptor (GHR) on many cell and organ types. Growth hormone signaling is initiated and mediated by this interaction. Growth hormone signaling brings about the production of another hormone, insulin-like growth factor-I (IGF-I or IGF-1), which is produced in the liver, adipose tissue and kidney and secreted into the bloodstream. About 75% of serum IGF-I is produced in the liver in response to growth hormone stimulation. Many disorders are caused by and/or associated with elevated growth hormone levels and/or elevated IGF-I levels in plasma and/or tissues including acromegaly, gigantism, retinopathy, macular degeneration, nephropathy, diabetes and cancers. The role of IGF-I in mediating many growth hormone effects is well recognized and the interrelationship is referred to as the growth hormone/insulin-like growth factor-I axis. In a normal feedback loop, IGF-I also causes the production of growth hormone by the pituitary to be reduced (i.e. negative feedback or inhibition).
Growth hormone is produced and secreted by a set of specialized cells in the anterior pituitary. Growth hormone has direct and indirect effects on many tissues, such as stimulating bone and soft tissue growth and influencing carbohydrate, protein, and lipid metabolism. Direct biological activities of growth hormone include receptor binding, internalization of the hormone/receptor complex, and activation of proteins involved in signal transduction.
GH Receptor
Protein and RNA transcripts for receptors of growth hormone (GHR) have been detected in many of the tissues influenced by the hormone. It was determined that a single molecule of growth hormone binds sequentially to two receptor molecules, forming an active complex. This complex, in turn, signals stimulation of other genes, including IGF-I. IGF-I, produced and secreted by the liver and other target tissues, mediates some of the indirect effects of growth hormone on growth and development. Other intracellular events occurring after the growth hormone/growth hormone receptor interaction include activation of tyrosine kinases such as Janus kinase 2 (Jak-2), which leads to phosphorylation and activation of other proteins including signal transducer and activator of transcription 5A and 5B (STAT 5A and 5B) and mitogen activated protein (MAP) kinase that, in turn, activate other proteins and genes.
The cDNA encoding the growth hormone receptor has been cloned from many species. The receptor consists of an extracellular hormone-binding region (exons 2-7), a single membrane spanning region (exon 8), and an intracellular region (exons 9-10). There are also multiple alternative 5' untranslated regions which are alternative first exons of the gene, in both the human and mouse transcripts. Growth hormone receptor has no intrinsic kinase domain, but the intracellular region plays a major role in the signal transduction process. A truncated form of the receptor, known as growth hormone binding protein (GHBP), lacks the transmembrane and intracellular regions of growth hormone receptor and is secreted into the serum. The truncated protein is produced by one of two different processes, depending on the animal species. In mice and rats, alternative splicing of growth hormone receptor precursor messenger RNA replaces the transmembrane and intracellular regions with a very short hydrophilic tail (encoded by exon 8A; 15, 16). In humans, cows, and pigs (among others), no alternative RNA splicing is apparent but instead the GHBP is produced by proteolysis of the growth hormone receptor. The function of the binding protein appears to be to modulate the level of circulating growth hormone.
Growth hormone receptor is expressed in many organs and tissues including liver, adipose tissue, muscle, cartilage, bone, tooth, kidney, eye, cardiovascular system, gut, reproductive organs, skin, brain, endocrine system and immune system.
The three-dimensional structure of the extracellular domain of growth hormone receptor has been established. It consists of two modules, each of about 100 amino acids, arranged as two sandwiches each with seven strands of beta-sheet. The secreted form of the extracellular domain of growth hormone receptor is the GHBP.
The growth hormone receptor is biologically responsive to growth hormone stimulation. JAK2 is the primary effector molecule for growth hormone receptor signaling. JAK2 is activated post growth hormone receptor dimerisation. When the growth hormone dimerizes its receptors, the JAKs are brought close together, and with proper alignment transphosporylate each other, leading to full activation. The intracellular targets for the JAKs include tyrosine residues in the receptor cytoplasmic domain itself, which in turn activate SH2 domains (STATS, She and SHP2). These may go on to activate the MAP kinase pathway, which regulates cell proliferation. JAK2 also phosphorylates and activates other signaling molecules, such as IRS-1 and -2 and phosphatidyl 3-inositol kinase, which are important parts of the insulin signaling mechanism and may account for the insulin-like actions of growth hormone. Activated JAK2 also phosphorylates STATS, and when activated, is involved in the transcription of a number of genes.
The Actions of GH Receptor Activation
Growth hormone receptor activation leads to many actions in many organs including the following outcomes in the following organs:
Liver:
Increased secretion of insulin-like growth factor-I,
synthesis of plasma proteins,
regulation of nitrogen balance enzymes,
increased carbohydrate synthesis/storage,
and increased fat breakdown;
Adipose Tissue:
Breakdown of fat stores;
Muscle:
Increased protein synthesis,
decreased protein breakdown;
Cartilage:
Increased height by increasing proliferation and differentiation of chondrocytes in growth plate;
Bone & Tooth:
Increased turnover of tissue, both synthesis and breakdown;
Kidney:
Increased sodium, bicarbonate and water retention;
Eye:
increased retinal neovascularization;
Cardiovascular:
Hypertrophy,
increased contractility,
stroke volume,
cardiac output;
Gut:
Hypertrophy,
increased amino acid, sodium, calcium, phosphate and B12 uptake;
Reproductive System:
Increased sperm production and motility,
increased accessory gland secretion in male,
increased number of follicles and ovulation rate,
increased follicular maturation rate,
increased milk production;
Skin:
Increased skin thickness and strength,
increased hair growth and thickness;
Brain:
Increased neuron proliferation and connectivity prenatally,
increased myelin formation,
improved long-term memory;
Endocrine System:
Increased insulin synthesis and secretion,
increased adrenal steroidogenesis;
Immune System:
Increased immune cell proliferation,
increased killing by monocytes, macrophages and NK cells,
increased antibody production
IGF-1
Downstream from growth hormone receptor in the growth hormone signaling pathway are IGF-I and IGF-I receptor. The insulin-like growth factors (IGFs) are important in proliferation. In particular, IGF-I and IGF-2 are ubiquitous polypeptides each with potent mitogenic effects on a broad range of cells. Molecules of the insulin-like growth factor type are also known as "progression factors" promoting "competent" cells through DNA synthesis. The insulin-like growth factors act through a common receptor known as the Type I receptor or IGF-IR, which is tyrosine kinase linked.
Particular proteins, referred to as insulin-like growth factor binding proteins (IGFBPs), appear to be involved in autocrine/paracrine regulation of tissue insulinlike growth factor availability (Rechler and Brown, Growth Regulation, 1992,2,55-68). Six IGFBPs have so far been identified. The exact effects of the IGFBPs are not clear and observed effects in vitro have been inhibitory or stimulatory depending on the experimental method employed. There is some evidence, however, that certain IGFBPs are involved in targeting insulin-like growth factor-I to its cell surface receptor. Also expression of IGFBP-3 is regulated by growth hormone.
The IGF-R is a tyrosine kinase linked cell surface receptor that regulates cell division, transformation and apoptosis in many cell types.
Disease states related to GH/IGF-1
If feedback regulation of growth hormone production is lost and the pituitary continues to release aberrant amounts of growth hormone, the level of insulin-like growth factor-I continues to rise, leading to bone growth and organ enlargement. The excess growth hormone also causes changes in sugar and lipid metabolism, which may lead to diabetes. Defects in the growth hormone signalling pathway often lead to abnormalities of stature and body and/or organ size. Mutations in the growth hormone receptor gene result in extreme short stature (Laron's syndrome). Excessive production of growth hormone can lead to acromegaly or gigantism.
Excess GH
Acromegaly and gigantism are related growth disorders wherein growth hormone excess, sometimes caused by pituitary tumor, causes progressive cosmetic disfigurement and systemic organ manifestations. It affects 40-50 per million people worldwide with about 15,000 sufferers in each of the US and Europe and an annual incidence of about 4-5 per million. It is initially characterized by abnormal growth of the hands and feet and bony changes in the facial features. Patients have reduced quality of life with overgrowth of the jaw, enlargement of hands and feet, deepening of the voice, thickening of skin, offensive body odor, articular cartilage problems, hyperphosphatemia, peripheral neuropathies, higher blood pressure, diabetes, heart disease, and cancer, and have a reduced life expectancy if untreated. The mortality rate is about twice that of the normal population due to cardiorespiratory and cardiovascular diseases, diabetes and neoplasia, particularly colon cancer. The goal of current treatment is to reverse the effects of the hypersecretion of growth hormone and normalize production of IGF-I which is elevated by about 50% in these patients. When effective, treatment moderates disease symptoms and disease-associated mortality.
Gigantism, the disease of excess growth hormone in children, is a rare disorder. In gigantism, excessive linear growth occurs whilst epiphyseal growth plates are open during childhood with growth hormone excess caused via a benign pituitary tumor. In both gigantism and acromegaly, all growth parameters are affected, although not necessarily symmetrically. Many of the growth related outcomes are mediated by elevated levels of serum IGF-I. Serum blood levels of IGF-I are elevated by about 50% in patients and reduction of serum IGF-I is used to monitor treatment
Treatments for acromegaly and gigantism involve the ability to lower the elevated IGF-I in plasma. This may be achieved by surgical removal and radiation therapy of the benign pituitary tumor but this is effective in only 50% of patients. Dopamine agonists such as bromocriptine mesylate or cabergoline may be dosed orally which is convenient but they only reduce growth hormone production and associated IGF-I sufficiently in 10% of cases. They also produce significant gastrointestinal and central side effects in 20-30% of patients. Also used in treatment of acromegaly are the somatostatin analogues such as Sandostatin or octreotide, which inhibit the release of growth hormone releasing hormone (GHRH) from the hypothalamus, and/or pituitary and thereby reducing production of growth hormone in the pituitary. This compound is effective in 60-65% patients with acromegaly but it must be injected under the skin every 8 hours or intramuscularly for effective treatment.
GHR Antagonist
Recently a growth hormone receptor antagonist, Trovert, also known as Somavert, Pegvisomant and B2036PEG, was shown in clinical trials to be effective in 90-95% of patients. Clinical trial experience to date shows a 10% drop-out rate and adverse effects such as liver dysfunction. Trovert is a growth hormone molecule with a 9 amino acid substitution with 4-5 pegylations to increase half life. Like all modified proteins it is immunogenic, with antibodies being made to Trovert within 1 month of dosing. This can impact Trovert's short and long term utility and makes dosing difficult to predict. Trovert was initially dosed once per month by subcutaneous (sc) administration, but current clinical practice suggests dosing will need to be once/day sc. Trovert interferes with growth hormone binding to its receptor but not the Growth Hormone Binding Protein (GHBP) fragment of the growth hormone receptor. GHBP binds growth hormone prolonging its action, which can be disadvantageous in conditions involving excess growth hormone and/or excess IGF-I. Pegylation may also impact on Trovert's long term safety profile.
Diabetes
Diabetes and its life threatening complications such as diabetic retinopathy and nephropathy are also disorders associated with growth hormone and/or IGF-I levels. First line treatment of these conditions involves controlling hyperglycemia. Drugs that control diabetes reduce the incidence of nephropathy by 60% and also reduce the incidence of retinopathy. However, about half of all diabetics are unaware of disease and therefore remain untreated, so diabetic nephropathy and retinopathy are likely to remain a major condition requiring other treatments. In retinopathy surgical ablative treatments such as laser pan-retinal photocoagulation are used but these remain incompletely effective and destroy retinal tissue, causing partial vision field loss. In type I diabetics ACE and All inhibitors decrease albuminuria excretion by acting on the kidney and in Type II diabetics the same inhibitors act locally on kidney and also decrease blood pressure to reduce the risk of death from kidney failure by another 50%. However, 20-30% of patients remain resistant to treatment with current glycemic control drugs and ACE drugs. There is thus a need for better treatments.
The underlying cause of diabetes, diabetic retinopathy and diabetic nephropathy may be insulin related hyperglycemia, but growth hormone and/or insulin-like growth factor-I excess is also important. Octreotide inhibitors of GHRH that decrease production of pituitary growth hormone, reducing systemic levels of growth hormone and IGF-I, and/or modulating local tissue levels show potential in the clinic. A study with octreotide by Grant et al., Diabetes Care, 2000, 2, 504-9) reducing sIGF-1 by 51% at maximally tolerated doses of octreotide 5000 ,Mg/day sc reduced the need for laser surgery in retinopathy patients to 1 patient out of 22 rather than 9/22 in placebo in a 15 month study. Also ocular disease was reduced to 27% vs placebo of 42% bordering on significance (P 0.06). Three human studies using octreotide at levels that reduced sIGFl 45%, about 20% and about 10% respectively were at least partly effective in clinical trials of nephropathy. The outcome reported by Serin et al. (JAMA, 1991, 265, 888-92) with 11 patients used high doses of octreotide in a 12 week study that reduced serum IGF-I by 45%. At the time it was stated to be the best effect observed on reducing glomerular filtration rate with a 22-33% reduction relative to placebo. This dose, however, was near maximally tolerated doses of octreotide.
Animal pathology model studies with octreotide and Trovert also support the view that agents that modulate the growth hormone/insulin-like growth factor-I axis are beneficial in the treatment of these diabetic conditions. Growth hormone and its receptor are implicated in the induction of glomerular hypertrophy and sclerosis in partial nephrectomy and diabetic nephropathy with somatostatin inhibitors octreotide and PTR-3173 (Groenbaek et al., /. Endocrinol, 2002, 172, 637-643 and Landau et al, Kidney International, 2001, 60, 505-512) and growth hormone receptor antagonist, G120K-PEG, a weaker version of Trovert, preventing complications in type I and Type II diabetic mice (Chen et al, Endocrinology, 1996,137, 11, 5136-5165; Flyvbjerg et al, Diabetes, 1999, 40,377-382, and Segev et al., /. Am. Soc. Nephrol. 1999, 10,2374-81). Growth hormone and its receptor are implicated in the induction of retinal neovascularization through IGF-I with somatostatin inhibitors octreotide and growth hormone receptor antagonist MK678, inhibiting retinal neovascularization in mice. MK678 reduction of neovascularization correlated with low serum IGF-I (Smith et al, Science, 1997, 276, 1706-9). Oxygen induced retinopathy in the mouse was also responsive to octreotide as reported by Higgins et al.,Exp. Eye Res, 2002, 74,553-9.
Macular Degeneration
Macular degeneration is also associated with elevated growth hormone and/or IGF-I levels. Age-related macular degeneration (AMD) is caused by deterioration of the central part of the retina, the macula, resulting in loss of detailed vision. Wet AMD, the less common form, is caused by leakage from new blood vessels growing behind the retina. The growth hormone/IGF-I axis is involved in formation of new blood vessels relevant to this condition and to diabetic retinopathy.
Cancer
Various cancers are also associated with aberrant growth hormone and/or IGF-I levels. Reduction of serum IGF-I by 20-50% using Trovert decreased tumor volume in breast cancer in animal models and helped in colon cancer, liver metastasis, and meningiomas (Friend et al, Proceedings llth NCI EORTC. AACR Symposium and Friend, Growth Harm. IGF Res., 2001, Jun: 11 Suppl A: S121-3). The incidence of breast, colon, prostate, and lung cancer is increased in individuals in the high normal range of serum IGF-I. There have been no clinical studies with Trovert in cancers. However, octreotide is indicated for gastro-pancreatic cancers.
Longevity
Longevity may also be improved with modulation of growth hormone receptor (Coschigano et al., Endocrinology, 2000, 141, 2608-2613). There was a significant increase in lifespan of nearly a year in double knockout animals with low levels of IGF-I and high levels of growth hormone.
Inhibition of Neuronal Differentiation
Another application to modifying levels of growth hormone and/or IGF-I via the growth hormone receptor may enable stem cell differentiation towards neural cell production as growth hormone inhibits neuronal differentiation of neural progenitor cells (Turnley et al., Nature Neuroscience, 1 Oct. 2002, published online).
Although the underlying roles in various disease or conditions may be different, the above conditions arise at least in part from incorrect levels of expression of local and/or systemic growth factors growth hormone and IGF-I and/or their receptors growth hormone receptor and IGF-R. In these situations, dopamine agonists, somatostatin antagonists, and growth hormone receptor antagonists targeting the proteins have been used and/or shown potenial
In reference to DatbTrue
-
5 minutes ago, MuscleDummy said:
Hey same user name same guy from NM, glad to see we have somewhere to go for this shit still. Looking forward to continuing to gain.
welcome MD,we did what we had to for everyone but we are back at it again and much better aswell

-
1
-
-
Body Fat Percentage Pics of Men & Women
 Lacking a mechanical tool, such as calipers, bod pod or other sophisicated devices, this alternative includes terminology and descriptions and I found the pics, especially of "real" people, to be extremely useful in estimating body fat %. Enjoy!!!
Lacking a mechanical tool, such as calipers, bod pod or other sophisicated devices, this alternative includes terminology and descriptions and I found the pics, especially of "real" people, to be extremely useful in estimating body fat %. Enjoy!!!
http://www.builtlean.com/2012/09/24/...age-men-women/
Body fat percentage is thankfully gaining more popularity as an effective marker of overall health and fitness instead of the BMI Index.
While I’ve written extensively about body fat percentage in numerous articles including Ideal Body Fat Percentage Chart, 5 Ways to Measure Body Fat Percentage, and Ideal Body Weight Formula among many others, I’m hoping this article will help tie everything together by creating visual representations of what a given amount of body fat looks like for men and women.
I searched thousands of images in order to create this article. Most of the images I purchased from stock photography websites, but others are in the public domain (at least I hope). If one of these pictures is copyrighted, please let me know and I will list proper attributions, or replace it if need be.
Body Fat Percentage Basics
To best understand the descriptions in this article and how the pictures were chosen, here are some basic body fat percentage terms and concepts that are helpful to learn:
Body Fat Percentage – is the amount of body fat (lb, or kg) divided by total body weight listed as a percentage. For example, a 180lb man with 30lb of body fat has a body fat percentage of 16% (30/180).
Body Fat Distribution – We all have different body fat distributions, or how fat is distributed across our body. For example, some women may have very little body fat on their abs, but a lot on their thighs and triceps, while others will have the opposite. Same thing goes with men, but most men carry fat in their stomachs. I tried my best to show pictures that highlighted the stomach region for men and the hips/thighs/stomach region for women.
Body Shape - Similar to body fat distribution is we all have different body shapes, so two different body shapes may have the same body fat percentage even if they don’t look like it. A classic example is a skinny runway model may have the same body fat percentage as a fit, athletic women.
Age – The pictures in this post assume ages of around 25-35 years old. Most body fat measurement devices will reflect higher body fat levels as the age increases. For example, a 20 year old man and a 50 year old man may have the same subcutaneous body fat measurement (fat under the skin), but the 20 year old may be 15% and the 50 year old will be at 20%. As we age, fat around the organs (visceral) and within muscle (intramuscular) tends to increase and most formulas take this into account.
Muscle Striations – As an individual becomes more defined, the actual muscle can be seen more clearly, which looks like thin rods, referred to as striations.
Vascularity – This is the appearance of veins in different areas of the body as body fat decreases.
Body Fat Pictures Of Men
Attachment 127645Attachment 127646
Body Fat Picture Descriptions Of Men
Body Fat Percentage Men 3-4%
Bodybuilders can drop as low as 3-4% body fat when preparing for bodybuilding competitions. This body fat level is characterized by extreme vascularity, so that veins are visible over just about every muscle in the body. There is clear separation between muscles, and striations visible on almost every muscle. The buttocks (I’ll spare you a back picture) even has striations, some vascularity, with little fat. If your buttocks doesn’t have any body fat, you’ve got VERY low body fat! Essential fat for a man is around 2%, which is the basic amount of fat a man needs for the body to function (fat protects internal organs in the chest and abdomen).
Body Fat Percentage Men 6-7%
Approximately 6-7% body fat for a man is a bit less extreme than competition bodybuilders, but it’s still hovering at a level that is not sustainable for most men. Around this level, or slightly less, the face becomes gaunt, and your family starts worrying about you. This 6-7% body fat level, which is achieved by many male fitness models when doing photoshoots, is characterized by muscle definition in all muscles and clear vascularity in most muscles including arms, legs, and even abs. Vascularity over the abs muscle is a sign of very low body fat. Clear separation of muscles as well.
Body Fat Percentage Men 10-12%
This is a sustainable level for most men where you should be able to see your abs, but they will likely not be as defined as a man in the 6-7% body fat range. This body fat range is the classic beach body look that most men want and many women love. While not very defined, there is separation between muscles, some muscle striations potentially in the shoulders, or arms, but striations are not showing on every muscle. Vascularity is typically limited to the arms, with a little possibly on the legs.
Body Fat Percentage Men 15%
The 15% body fat level is usually within the “lean and fit” category in most body fat percentage charts. The outlines of muscle can be seen, but there is no clear separation between them. Vascularity is usually a bit more limited as are muscle striations, which are typically covered by a thin layer of fat. The overall shape is still there, which can create an aesthetic appearance despite less muscle definition.
Body Fat Percentage Men 20%
Separation between muscles starts to blur, almost no vascularity, or striations can be seen, typically there is a small stomach pouch of fat, the look is “soft” but not very round. Most guys I come across in NYC are within the 20-25% body fat range. Other parts of the country, or world, that range may be skewed higher or lower. A 5’11”man who weighs 180lb and has 145lb of lean body mass (the average) will have 20% body fat.
Body Fat Percentage Men 25%
There is little to no separation of muscles, no vascularity, or muscle striations, waist begins to increase quite substantially with a waist to hip ratio as high as 0.9 (waist circumference/hip circumference). So a 5’10” man may have a 36+ inch waist. This man may have a little neck fat, but may not look like he has 25% body fat in normal clothing. Over 25% body fat for a man is considered obese, and over a 40 inch waist is considered abdominal obesity.
Body Fat Percentage Men 30%
There is more fat all around the body at the 30% level including waist, back, thighs, and calves. The waist looks larger relative to the hips, and the stomach will likely be protruding over the waist noticeably. There is no muscle separation.
Body Fat Percentage Men 35%
As men get heavier and heavier gaining more fat, most of the fat is funneled right in the stomach. The 35% level is characterized by more significant protrusion of stomach fat over the waist. This is the beer gut kind of look. Waist circumferences can be 40+ inches for a man with 35% body fat.
Body Fat Percentage Men 40%
Similar to the 35% level, even more fat accumulates in the stomach and waist region, so that waist sizes can approach 45 inches, or more. At this level, basic every day activities like walking up stairs, or bending over to pick something up becomes increasingly difficult. This body fat level is approaching morbidly obese, which is characterized by a BMI over 35. To put it in better perspective, a 5’11” man who weighs 270lb and has 160lb of lean body mass has 40% body fat.
Body Fat Pictures Of Women
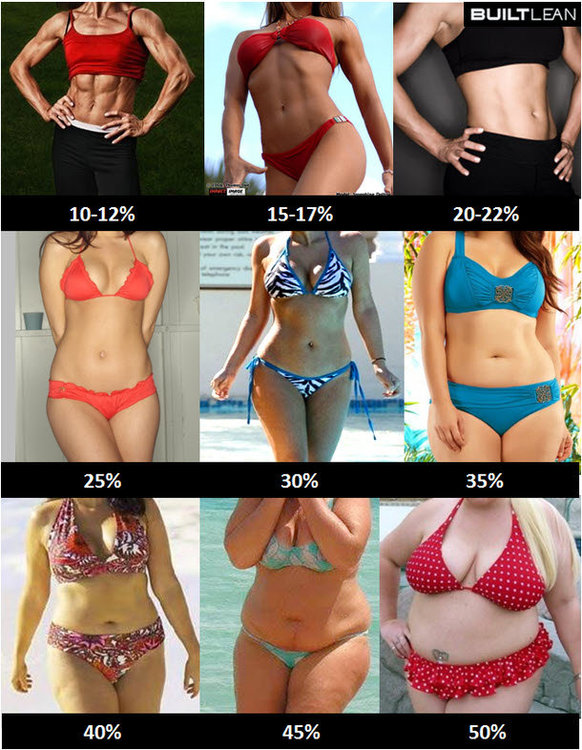
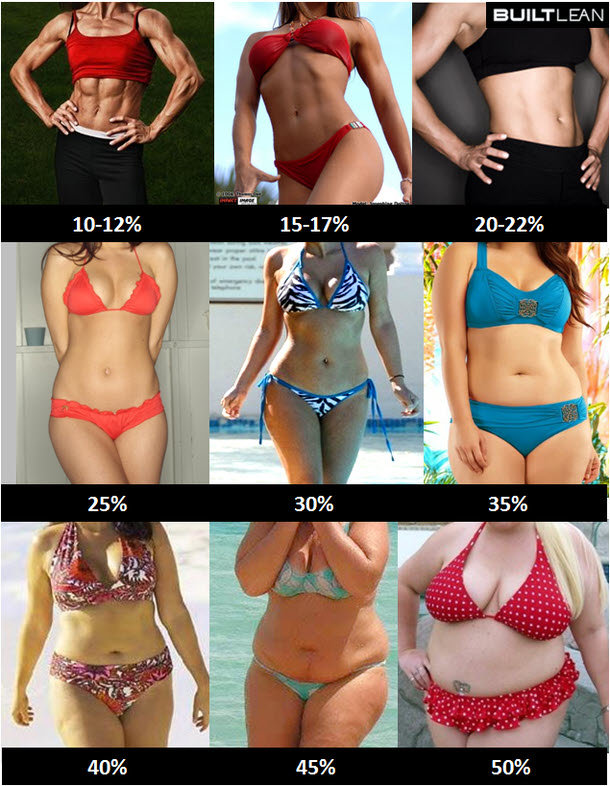
Attachment 127647Attachment 127648
Body Fat Picture Descriptions Of Women
Body Fat Percentage Women 10-12%
This is an extremely low body fat level typically attained by female bodybuilders. Essential fat for women is round 8-10% compared to 2% for men. Why the difference? Women have more fat in breast tissue and the area surrounding the uterus. This level of body fat is not considered safe, or healthy for women who will be unable to menstruate. Striations of muscle, separation between muscles, clear vascularity are all noticeable at this level. The women in the photo is likely at the higher end of the range at 12% body fat because she is not too vascular.
Body Fat Percentage Women 15-17%
This is still considered a very low body fat for women, which is similar to the 6-7% body fat for range men. Many bikini and fitness models will reach this body fat level and some may not be able to menstruate. Muscle definition in the abs, legs, arms, and shoulders is apparent, there is some vascularity and some separation between muscles. Hips, buttocks, and thighs generally have a little less shape because of the low body fat.
Body Fat Percentage Women 20-22%
This is body fat percentage is usually in the “fit” category of most body fat charts and is typical of many female athletes. Some definition in the abs is apparent, there is body fat on the arms and legs, but it’s not too pronounced. There is minimal, but some separation between muscles.
Body Fat Percentage Women 25%
This is on the low end of what’s average for most women and is characterized by a shape that is neither too slim, nor overweight. Curves in the hips are usually more apparent along with more fat in the buttocks and thighs. A 5’4” women who weighs 130lb and has 97lb of lean body mass has 25% body fat.
Body Fat Percentage Women 30%
While most men have fat funnel into their stomachs, as the body fat of most women (but certainly not all) increases, this fat tends to accumulate in the hips, buttocks, and thighs. At 30% body fat, the hips, thighs, and buttocks are more pronounced and round. This is considered the high end of average for women in many body fat charts.
Body Fat Percentage Women 35%
The hips become even wider at this level of body fat and the face and neck will appear rounder and more full. Hip circumference can start approaching 40+ inches and waist circumference of 32+ inches. Some belly fat may start protruding over the waist as well.
Body Fat Percentage Women 40%
The hips and thighs grow larger so that hip circumference can reach 42+ inches, waist of 35 inches, and thighs over 25 inches.
Body Fat Percentage Women 45%
The skin may begin to lose its smooth appearance as more and more fat accumulates. Hip Circumference can may reach 45 inches+ and waist circumference 35+ inches. The hips may become noticeably wider than the shoulders.
Body Fat Percentage Women 50%
The will likely look like it has dimples more fat accumulates. Hip Circumference can may reach 45+ inches and waist circumference 40+ inches and thighs above 30+ inches. The hips will likely be noticeably wider than the shoulders. To put it in better perspective, a 5’4” women who weighs 200lb and has 100lb of lean body mass has 50% body fat.
Given how confusing measuring body fat percentage can be, I hope seeing these body fat percentage pictures was helpful!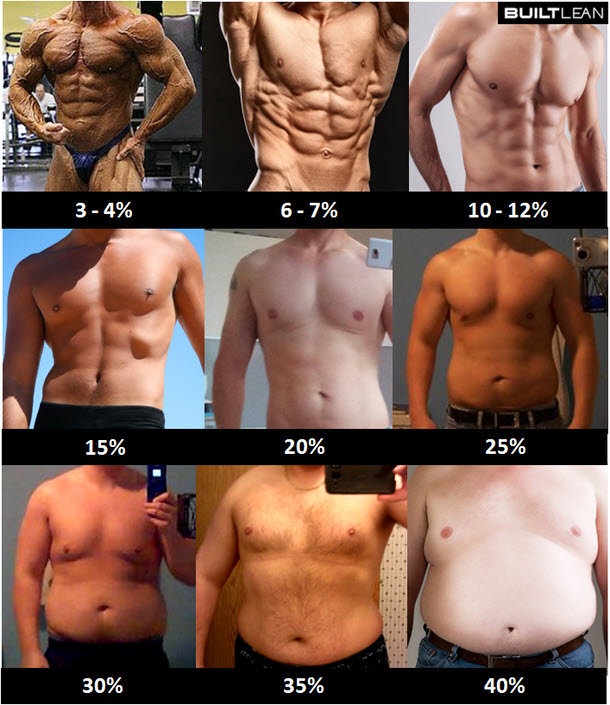


-
3
-
-
2 minutes ago, Physlifter said:
Looks nice in here
I'll think i'll come and stay awhile!eh,glad you made it sir
-
http://swole.me
https://www.eatthismuch.com/
Pretty cool. Probably been around awhile but just ran across this.
Click “show intro” at top to see instructions-
7
-
-
What is 'GI' and a List of Common Foods
'GI'....The term is tossed around often as we all have made low GI carbohydrates a staple of our diet. Yet, how many of the newer individuals to our lifestyle really understand what 'GI' is, how to implement or why for that matter?..Considering this I figured I'd put together this thread for info's sake
What is 'GI'?
'GI' stands for glycemic index. The Glycemic Index is a numerical Index that ranks carbohydrates based on their rate of glycemic response (i.e. their conversion to glucose within the human body). Pure glucose is given an arbitrary rating of 100 as a reference point and all other carbohydrates are rated from 0 onwards. Any carbohydrate with a rating below 55 is considered a "low GI food", and conversely any food 70 and up is generally considered a "high GI food"
Why Are Low 'GI' Foods Important?
Our bodies perform best when our blood sugar (blood-glucose) levels remain at a relatively constant level, supplying our bodies with equal amounts of fuel throughout the day. For our lifestyle choice it is important to have an equal, constant stream of glucose in order for muscle glycogen conversion. Low 'GI' foods are less rapidly absorbed by the body than foods with high 'GI' and therefore provide a more constant stream of fuel.
Is The Glycemic Index the Only Tool To Measure Carbs?
Although the Glycemic Index is our most useful tool when discerning which carbohydrates to eat, it is not our only one. Of the other branches which apply to the 'GI' the Glycemic Load is the most useful. When you intake carbohydrates it is not only important to note what the rate of glucose conversion will be, but how much total carbohydrate you are taking in, this is where GL comes into play. Glycemic load is used to determine (with GI) what your bodies total glycemic response will be. It is measured by dividing the GI by 100 and multiplying that by the net carbs (net carbs are equal to total carbs minus dietary fibre)
(GL=GI/100 x Net Carbs)
Should High GI Foods Be Completely Avoided?
Although low-GI, complex carbohydrates should be the vast majority of your caloric intake for carbs to ensure consistent glycemic response, there are times when a rapid increase in blood sugar is desirable. For this purpose some individuals choose to intake high GI foods after strenuous activity in hopes of causing an insulin spike in order to move glucose to the muscles to be converted to glycogen. Though not all agree with this method it has been utilized successfully, though the risk for adipose storage can be an issue. (in excess)
Is GI Fail-Proof
Absolutely not, as with any measuring formula the Glycemic Index is prone to some fallacies. Some of these limitations are noted below
Wide Spectrum Of Measurements
Normally, the reported GI value of a carbs is the average of many test results. Because of this there are often conflicting reports on the GI of common foods. For example the common potatoe has been reported as low as 55 and as high as 100.
Individual Glycemic Response
Each one of our bodies is unique in it's processing of the food we intake. Each individuals rate of glycemic response, and conversely, insulin response is different, so although the GI is a useful tool it should not be religiously followed. The best method of utilizing the GI is to experiment to discover what your own bodies GI response is to craft the perfect "low GI diet" for you.
Preparation
The GI of any given carbohydrate can be modified, sometimes significantly, by the method of preparartion. Any significant processing such as cooking, boiling, baking, or grinding may alter the GI of the food. Also, combination with other foods may also alter the initial GI of both carbs. When foods are combined at times a 'mixed GI rating', an average of both the foods GI's can be implemented to rate the entire meal. However, this can also be misleading as often times the foods will have a synergistic effect and cause an overall higher glycemic response than either individual part may have had.
How Should I Best Implement the GI
Quite simply by using it as a guideline, and determining what is best for you. Many factors, such as the ones listed above have to be taken into account when determining which carbohydrates will most effectively allow you to put on LBM whilst keeping fat down. Consider your roomate who eats Burger King five times a week, drinks a two litre of Cola a day, and puts in minimal effort at the gym, yet still has an equal physique to you. Obviously, your individual insulin/glycemic resonse times greatly differ from eachother, and therefore have to eat greatly differing diets to maintain the same body. As said above a specifically tailored diet, implementing low GI foods, will allow you to most effectively use the Glycemic Index..
Common Food Listing
Food Glycemic Index
Breads
Bagel, white 103
Hamburger bun 87
Melba toast 100
Oat bran bread 68
Rye kernel bread 66
Pumpernickel 71
Rye flour bread 92
Linseed rye bread 78
Wheat bread, white 100
Wheat bread, high fibre 97
Wheat bread, gluten-free 129
Wheat bread, wholewheat 99
Wholewheat snack breads 105
Pita, white 82
Mixed grain bread 64
Breakfast cereals
All-bran 60
All-bran with raisins 74
Cocoapops 110
Cornflakes 119
Cream of wheat 100
Muesli 80
Oat bran 78
Oatmeal 87
Puffed wheat 105
Rice bran 27
Rice crispies 117
Shredded wheat 99
Special K 77
Cereal grains
Barley, pearled 36
Barley, cracked 72
Barley, rolled 94
Bulgur wheat 68
Couscous 93
Maize meal 97
Millet 101
Sweet corn 78
Rice, white 81
Rice, Basmati 83
Rice, brown 79
Rice, instant, boiled for 6 min. 128
Rice, instant, boiled for 1 min. 65
Rice, parboiled 68
Rice, wild 81
Rye kernels 48
Tapioca boiled with milk 115
Cakes and biscuits
Butter biscuits 79
Cake, angel food 95
Cake, banana loaf 67
Cake, sponge 66
Coffee cookies 113
Crispbead 116
Croissant 96
Crumpet 98
Digestive biscuits 84
Doughnut 108
Graham crackers 106
Maizena cookies 95
Muffins 88
Oat cookies 79
Pastry 84
Pizza base with cheese 86
Rice cakes 117
Rye crispbread 93
Shortbread 91
Waffle 109
Water biscuits 102
Wheat crackers 96
Drinks
Cold drinks, sweetened 97
Cordials 94
Gatorade (energy drinks) 136
Fruit and Fruit Juices
Apple 52
Apple juice 58
Apricots, fresh 82
Apricots, canned in syrup 91
Apricots, dried 44
Banana 76
Cherries 32
Fruit ****tail 79
Grapefruit 36
Grapefruit juice, unsweetened 69
Grapes 62
Kiwi fruit 75
Mango 80
Orange 62
Orange juice 74
Pawpaw 83
Peach, raw 40
Peach, canned 79
Pear, raw 51
Pear, canned 63
Pineapple, raw 94
Pineapple juice 66
Plum 34
Raisins 91
Spanspek 93
Sultanas 80
Watermelon 103
Legumes
Baked beans, canned 69
Beans, dry 40
Broad beans 113
Butter beans 44
Chickpeas 47
Chickpeas, canned 60
Kidney beans 42
Kidney beans, canned 74
Lentils 41
Lentils, green, canned 74
Lima beans, frozen 46
Soya beans 25
Soya milk 43
Split peas, boiled 45
Milk and dairy products
Ice cream 87
Ice cream, low-fat 71
Milk, whole 39
Milk, skim 46
Milk, chocolate 49
Milk, chocolate (artificial) 34
Custard 61
Yoghurt, low-fat, fruit, sweetened with sugar 47
Yogurt, low-fat, artificially sweetened 20
Yoghurt, plain 51
Pasta
Fettucine 46
Gnocchi 95
Instant noodles 67
Macaroni 64
Macaroni and cheese 92
Ravioli, meat filling 56
Spaghetti, protein-enriched 38
Spaghetti, white 59
Spaghetti, durum 78
Spaghetti, wholewheat 53
Vermicelli 50
Snacks and sweets
Jelly beans 114
Lifesavers 100
Chocolate 70
Chocolate bars 91
Energy bars 81
Maize snacks 105
Muesli bars 87
Popcorn 79
Potato chips 77
Peanuts 21
Pretzels 116
Soups
Bean soup 92
Green pea soup, canned 94
Lentil soup, canned 63
Split pea soup, homemade 86
Tomato soup 54
Sugars
Honey 104
Fructose 32
Glucose powder 138
Glucose tablets 146
Maltose 150
Sucrose (table sugar) 92
Lactose 65
High-fructose corn sugar 89
Maltodextrin 107
Vegetables
Beetroot 91
Carrots 101
Parsnips 139
Peas, dried 32
Peas, green 68
Potato, instant mash 118
Potato, baked 121
Potato, new 81
Potato, boiled 80
Potato, boiled, mashed 104
Potato, microwaved 117
Potato chips, deep-fried 107
Pumpkin 107
Sweet corn 78
Sweet potato 77-
3
-
 1
1
-
-
Hardgainer? Can't gain weight? READ THIS!!!
Diet is 75% of bulking up IMO. You can lift like Ronnie Coleman, but bottom line you will not grow any muscle without the calories behind it for bulking. Simple biology and one equation---->
Calorie balance=Calories in - Calorie expenditure
If you aren't gaining weight, you are not in a positive calorie balance so you need to either cut out all cardio, eat more, or both. Eat more calories than you burn, you will gain weight; eat less calories than you burn, you will lose weight. The kind of weight you gain or lose is dependent on your macronutrient breakdown, timing of meals, training, cardio, etc. Try adding up your calories using the links at the bottom of the page, many people who think they "eat all the time" actually eat under 3000 calories per day, which is very low for a bulking diet. Get used to eating frequently also, like every 3 hours tops. The only time I was hungry on my last bulker was right when I woke up in the morning. Remember: an appetite is not necessary to eat. You need to get used to eating what/when you MUST, not what/when you want.
There are two ways to bulk: A clean bulk (slower, but leaner gains) and a dirty bulk (faster gains, more fat storage if metabolism isn�t fast) The main difference is that on a clean bulk, you NEVER eat carbs and fats together. Milk is bad for this reason. Eating carbs and fats together causes almost all of the fat to get stored instead of used for energy. Don�t eat carbs in your last 2 meals of the day because they get stored as fat while you sleep. Eat at least 40g protein with every meal, and make meals either protein/fat or protein/carb.
PWO=Post Workout, the most anabolic (muscle building) time in anyone�s day is the half hour following a workout. It is best to use a fast-acting protein like Whey. Your muscles soak up protein like a sponge. It is also useful to eat twice as many carbs as protein to help shuttle the proteins to the muscles. The PWO shakes I use are
---50g Optimum Nutrition Whey
---50g Dextrose (Corn sugar, causes an insulin spike to increase absorption of protein)
---50g Maltodextrin (Powdered complex carb supplement)
Some people prefer to drop the maltodextrin and just do 100g of dextrose. Try both and see what works for you.
Eating approximately every 2.5 to 3 hours is good for 3 reasons�
1. You can eat more calories in a day if your meals are smaller. Its easier to eat 600 calorie meals 6 times a day then it is to eat 1200 calorie meals 3 times a day.
2. Your body can only digest so many calories at a meal, and the rest gets stored as fat. Lowering the amount of food eaten at one time reduces the �extra� over what you need.
3. Muscles start to catabolize (break down) if they are without protein for 3-4 hours unless you are sleeping. Hell, when I'm bulking I drink a milk/casein shake when I get up to piss at night.
For all you 130-150 pounders thinking about taking steroids... re-evaluate your diets. If you can't gain weight naturally, steroids aren't going to do anything for you except shrink your balls. Think about it... raw materials to form muscles have to come from somewhere right? They don't just appear out of thin air. Calories are the bricks that are building your house.
Try eating 300g protein, 400g carbs, and 150g fats.
You will grow.
A couple useful links
1) www.fitday.com <----Huge database of foods, can look up pro/fat/carbs and calories on them.
2) http://www.ntwrks.com/~mikev/chart1.html <------Basically the same
3) http://www.bodybuilding.com/fun/berardi41.htm <----- An equation that you
plug in your weight and bodyfat percentage and it will tell you how many calories you need to eat every day to grow.
If your diet is "all that and a bag of chips", and you STILL weigh 140 pounds dripping wet, either you have a SERIOUS thyroid problem or your training sucks. Remember "The Big 5" - Squat, Deadlift, Row, Bench, Military.
GET BIG!-
6
-
-
Very happy to hear about you being sober. Wish you much success on your bodybuilding journey
-
28 minutes ago, Twistert said:
Names Twister been back at lifting since January 2018 after having gone through some medical issue NM was great help hope to see everyone
Hope you are full recovered,welcome to the board
-
1
-
-
15 minutes ago, eazy57 said:
I'm a former NM member.
Nearing 50... been lifting since I was 38.
I'm a member of other forums.
Here's hoping this one sticks around.
Welcome Eazy,this board will definitely stay. Thanks for joining us
-
1
-
Contest prep for Women
in Bodybuilding and Training Talk
Posted
Contest Prep
by Allen Cress
There are many people out there who call themselves bodybuilders, but in my opinion, unless you have attempted to take the stage at least once in your life, you are just a weightlifter. There is a big difference between having a physique with some visible abs that looks good on the beach and the body that you see in competition, with striated glutes, paper-thin skin, and veins like you’d see in an anatomy chart. Many have attempted to step on stage, and many have failed. In my mind, that’s what separates a wannabe bodybuilder from the real deal.
Bodybuilding isn’t for everyone, and for some it just isn’t in the cards due to body structure and genetics. You don’t necessarily need to have superior genetics like Jay Cutler to compete, but contest prep does require discipline, hard work, consistency, and the drive to do what it takes to get results. At the end of the day, genetics (and the judges) may determine the on-stage winner; however, the fact that you may not receive a trophy doesn’t mean you are not a personal winner as long as you did everything possible to be your best on that day. As I tell my clients, if you enjoy the process and the challenge, then you have already won.
Where do you start? One general recommendation I make is to hire qualified help. Even with the information in this article, which is written in a general format, there are too many individual differences among potential competitors that must be addressed. An expert will be able to hone in on your particular body and how it works, and then will be able to apply tried-and-true principles to achieve specific results while avoiding the traps and pitfalls that can occur during contest prep. Also, a professional will provide an objective viewpoint and will be able to help you keep your mind on the right path; as the diet progresses, it becomes as much a mental challenge for some as a physical one.
The Diet:
A lot of bodybuilders believe there is only one single process to follow to get ready for a show. Most pick a certain number of weeks before the show to start dieting, usually 12-16 at minimum, and then just gradually drop their calories as the show gets closer. How early you should start your diet depends on your current condition and how much fat you are carrying. A good rule of thumb is to give yourself one week for every percentage point of body fat. Therefore, if you have roughly 12% body fat, start at 12 weeks out; if you are over 16% body fat, start at 20 weeks out.
There are also many bodybuilders who still follow outdated and useless practices during prep such as carb depleting and then reloading the week before the show; all that does is risk damage to the physique. I like to use methods that are based more on science and in-the-trenches experience and not merely on tradition. Always plan extra time for contest prep to ensure optimum fat loss and retention of muscle mass. Specifically, you want to maintain a relative calorie deficit rather than an absolute calorie deficit (an important point I learned from Scott Abel). The reason for this is that in an absolute calorie deficit, an athlete can and almost always will lose muscle mass, which we would prefer to avoid at all costs. In an absolute caloric deficit, the body will be more stubborn about giving up fat because it is in starvation mode, which is roughly 750-1000 calories below an individuals BMR (Basal Metabolic Rate). In this state, the metabolism will protect fat storage at the expense of muscle in order to maintain energy expenditure.
For any diet, and especially for contest diets, a better approach is to use a relative caloric deficit in which an individual begins the diet at or near his normal BMR, which is the rate at which the body burns calories while at rest. Once the BMR has been established, the diet begins. There are various methods that can be used to prepare for a contest…the particular approach all depends on a person’s current needs state, how they have been eating up to that point, and their current condition. Some of these methods are: 1) staggering calories (one of my favorite methods), 2) carb cycling, or just a 3) a steady-state approach at or near the BMR, while introducing fat burning activities (such as a structured training program and cardio) to create a fat-burning machine rather than a fat-storing machine.
So how do we figure out a person’s BMR? There are some good equations out there, but to keep things simple, just take your bodyweight times 12 or 14 if you are in decent shape (below 14% body fat) or your body weight times 10 if you are on the fatter side (above 15%). Next, subtract 300-500 calories from that number, depending on how much fat you have to lose. There are several factors that influence the BMR, including gender, hormonal levels, age, height, and background. Therefore, it would be useful to have a record of a few days worth of eating in order to poinpoint an individual’s current caloric intake and how closely it matches their calculated BMR. Once calorie consumption is assessed, then we proceed to choosing an appropriate diet strategy. I recommend breaking the calories up into five, six, or even seven evenly spaced meals throughout the day. In this way, the body is more easily able to process smaller amounts of food efficiently and to keep insulin levels steady.
Once the general eating strategy is set, it is then necessary to structure the diet in terms of fat, carb, and protein percentages. One point I want to get across immediately is that in a calorie deficit (as in a pre-contest diet), there will be no predisposition for your body to store fat from ANY energy source (carbs, fat, or protein). Therefore, when dieting, don’t be concerned that a certain energy source may make you fat (the usual targeted source is carbs); instead, focus your sights on determining the best strategy to optimize fat loss while insuring retention of your hard earned muscle. Carbs and fats are the protein-sparing energy sources– enough of these must be present in a diet so that protein can be used to build and rebuild tissue. If not, the body will use protein for the production of energy at the expense of rebuilding tissue.
A word on carbs: Carbs are not the enemy, but too much insulin may be a problem when trying to get ripped on a diet. The problem is that too much insulin and too little insulin can both result in feelings of hunger. Therefore, to control insulin levels, we should monitor physiological feedback after meals. If there is too much insulin, the body feels tired and the mind sluggish. If insulin is low, the body feels hungry, but focus and concentration remain clear. Finding a balance between these two situations then becomes a matter of tweaking the meals during a diet. Someone who feels tired and lethargic after a meal may be consuming too many calories at that particular meal. If he feels hungry, but is still focused and alert, then his body is in a fat burning mode. As time goes on most bodybuilders get used to the hunger…it’s just part of a typical contest prep!
Getting back to macronutrients, how do we decide the ratios of proteins, carbs, and fats? As an example, let’s take a 200-lb client. Protein needs would be roughly 275 grams, as I like to keep protein around 45-50% of total calorie intake during contest diets. Because his BMR would be around 2400 calories, according to our calculations, I would recommend that 50% of that should consist of 300 grams of protein (just take 2400, multiply by .50, then divide by 4). Now there are 1200 calories left to divide between carbs and fat. Using a carb-based diet as an example, I would keep carbs at 35-40% and fat at 10-15%. I have gotten many competitors into ripped contest condition using this model. In terms of fat loss, you should monitor bodyweight and the image in the mirror each week (the mirror will always overrule the scale weight) as well as your body’s feedback on hunger, focus, energy levels, etc.. Remember, this is one of many possible ways to diet for a contest, and it always comes down to an individual’s physiology. This is one of the best parts of what I do–manipulate and coax the body to come in shredded and watch it all unfold in front of me.
Also keep in mind that if the body is in a fat burning mode, water intake needs to be increased as well. During diet periods, more body fluids will be lost and replenishment becomes crucial. Proper fluid replenishment and electrolyte balance is important at this stage to maintain cell integrity and intracellular water levels. Therefore, sodium ingestion should also be kept quite high through the whole prep by using sea salt and certain condiments.
After you have taken all of these variables into consideration and have set a plan into action, you can then and only then look for other factors that may influence performance. Finding the right training protocol and minimizing stress levels are factors outside of the diet that can contribute positively or negatively to performance. The others, of course, are supplements and drugs. Too many readers already rely too heavily on pharmacological influences so I will not go into that subject. However, supplements can be put to use in pre-contest dieting. Products are called “supplements” for a reason–they supplement diet and training, but they do not take the place of them. Supplements exist to aid the process of fat loss and muscle retention but they will not replace bad training, coaching, or dieting, and will not fix what is wrong with your overall protocol.
Cardio:
When it comes to cardio, the more fat you have to lose, the more cardio you may need to do. Keep your cardio sessions at 25-45 minutes; longer sessions will cost you hard earned muscle. If you have a lot of fat to lose, the key is to start cardio at the same time as you start dieting. The problem most competitors have is that they tend to throw the kitchen sink at themselves from the start, whether it be cardio or diet. If you start out at six 1-hour sessions per day and plateau at eight weeks left, where do you go from there? Yes, you would initially lose a lot of weight, but once you hit that plateau, you have no option but to go to extremes. Two sessions per day on top of workouts? You want bodybuilding to add something positive to your life, not consume your life. Furthermore, if you go to these extremes, the after-effects once the contest is over could be dangerous, and this is something you want to avoid as much as possible. So you want to get the most out of the least when it comes to cardio—add it only when needed. I would not recommend you start with more than three sessions a week at 30 min each unless you are completely out of shape.
Keep your cardio at an easy-to-maintain pace. The rule of thumb is that you should be able to maintain a conversation but still build up a sweat. You are a bodybuilder, not a runner; save the high intensity stuff for your workouts and keep cardio at a comfortable level. Now I know some individuals like HITT, but for the most part, once you are a month or so into contest prep, you will more than likely end up burning off muscle with this approach. If you want to do it for the first few weeks, that’s good, just be cautious. The time of day at which you do your cardio depends on your lifestyle and other factors. Forget this idea that “first thing in the morning on empty stomach” is absolutely necessary. That may be the absolute best-case scenario, but if you don’t have a good bike or treadmill at home, and you need to drive to the gym or you do your cardio after training, it’ll be fine. Don’t sweat the small details, just maintain consistency with your diet and training program.
First of all, I want to point out that if you didn’t put in the hard work and a good plan to get ripped ahead of time, then no amount of water manipulation, fat loading, or carb loading is going to work in the end. I often hear competitors say that they were just holding water—no, you were just not lean enough, period! If you are shredded, then proper loading can help you to look fuller and dryer in order to present the best package possible on stage.
What you do with your water intake depends on how you will be peaking. If you carb load, water manipulation will have to be different than if you fat load. For carb loading, you need to know that carbs require roughly three grams of water for one gram of carbs in order to load into the muscle cell. For simplicity, let’s say you are loading 400 grams of carbs, which would require 1200 grams of water to load into the muscle. To help with drying out, instead of taking in 1200 g of water, you take in 700 g of water. The body will take the rest of the water needed from its subcutaneous stores. Unless a client needs to make weight, we would typically start loading on Wednesday (Saturday being the contest day) and taper on Thursday; that way, we have some wiggle room for adjustments come Friday and Saturday, depending on how the client is looking. Therefore, you should decrease water as you decrease carb intake, but you should never completely cut water if you are just carb loading. Also, when you carb load you should use carb sources such as potatoes, rice, oatmeal, and rice cakes and not simple sugars. All those will do is cause bloating and water retention.
Another method, and one I use more often, is fat loading. Carb loading can work and work well for an individual with a higher metabolism, but for those more sensitive to carbs, it may be much harder to peak and keep water under control. Instead, fat loading can be done by increasing calories on Wednesday and Thursday (using good fats such as natural peanut butter, whole eggs, olive oil, and red meat) with minimal carbs at a couple of meals as well as keeping water intake low on the day of the show.
Alternatively, this can also be accomplished by taking in simple sugars along with very high fat foods using the correct timing. I learned this method when working with Scott Abel. You must cut out water completely for this approach to work, usually around 12 hours or so before the contest, in order to get rid of the little interstitial water you may have and to make room for fat loading. But first, before you cut your water, you need to take in as much water as you can starting on Tuesday and leading up to Friday. This will send the message to your body to turn off ADH (anti-diuretic hormone), which will ensure that you will continue to lose water even after you stop taking in fluids. Tapering off your fluid intake with this method is a huge mistake because that is what turns on ADH; as less water comes into your body, it responds by trying to hold and store its own water. The result is unwanted water retention. A good rule is that if you are on point conditioning-wise, you shouldn’t need to dehydrate for more than about 20 hours max. You should use foods such as prime rib, fries, cheesecake, nuts, pancakes, and even candy bars along with regular diet foods. If you are plenty dehydrated, after prejudging is over, then a diet soda or two will help fill out the muscles. Just make sure you have them between meals and not WITH your meals, and only have them if you look like you are getting flat. Remember, timing is everything.
Now if you are a novice and you are ripped and ready to go but are unsure about the peaking methods, don’t change a thing…if it ain’t broke, don’t try to fix it!. Don’t take a chance (as so many bodybuilders do at the last minute) if you truly don’t know what you are doing. To take months to prepare for a contest and then risk it all by trying methods you have no experience with is just not worth it. Fat loading and carb loading both work and work well, but they are not foolproof. This is where expert advice comes into play.
So, to sum it all up, here are the take-home points:
• Determine your timeline (err on the side of longer).
• Select your diet approach.
• Listen to your body and be objective (which is harder than you may think).
• Add in cardio only when needed.
• Be ready at least 1- 2 weeks prior to the contest.
• Don’t use ANY peaking method if you don’t know what you are doing.
• Don’t go to extremes. No contest is worth screwing up your body.
• Work hard and be consistent!
The best advice I can give is to hire a coach to guide you on this journey. It takes all the stress out of the process, and you will also learn things along the way. No two contest preps are ever the same, and prep even shifts from contest to contest as your body changes. A good coach will assess how your body works and will know when to make changes based on your feedback. Good luck and get yourself up on that stage!