

method_air
-
Posts
38 -
Joined
-
Last visited
-
Days Won
1
Everything posted by method_air
-
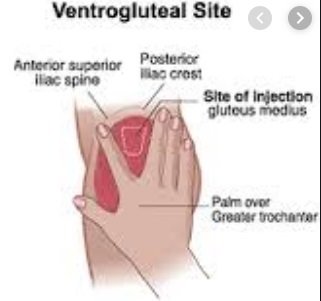
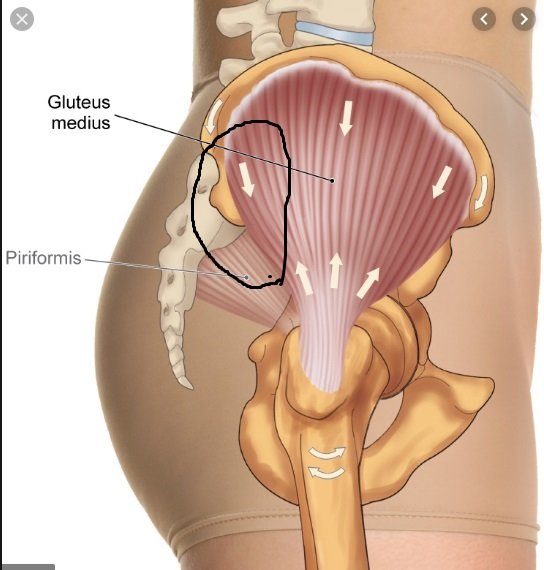
The greater part of the circled area of the image is in fact the glute medius muscle you reference. I'm not a fan of injecting into the anterior/ventro glute medial area, as my internal hip rotators are extremely thick. There will always be idiosyncrasies depending on what works for your anatomy. If one merely goes by the textbook, it says:
-
This is really insightful. It's the elephant in the living room.
-
Bad/Bunk Batch Test E? Crazy PIP 2-3 days after...
topic replied to method_air's mackmack403 in Steroid (AAS) Discussion
If it was from the ester, why were there no significant issues with his first few shots? -
Bad/Bunk Batch Test E? Crazy PIP 2-3 days after...
topic replied to method_air's mackmack403 in Steroid (AAS) Discussion
The advice is sound, however, there was nothing in Mack's posts to suggest that he wasn't already aware of this basic protocol. -
Feel for the muscular area above and behind the hip socket, and below the crest of the illiac, as per the approximate area shown in the attached image.
-
Bad/Bunk Batch Test E? Crazy PIP 2-3 days after...
topic replied to method_air's mackmack403 in Steroid (AAS) Discussion
>>400mg Test E weekly pinning 2x /week with a 23G 1'' I re-iterate everything said here, so: 1. don't inject in your quads 2. pin more frequently with smaller amounts 3. use a 25G "1, or maybe even 30g insulin syringes if you pin everyday 4. inject very slowly, carefully and aspirate 5. don't inject anywhere near an inflamed muscle 6. open a dialog with your source -
With due respect, the AI doses Rand mentions could crush estrogen for some. Primo, DHB, Masteron etc. might be equally effective, with respect to estrogen management. However, unlike arimidex, masteron is probably not medically prescribable in these cases.
-
Right, but oil (or anything else) could have an entirely different reaction. This might be unrelated, but still worth considering: https://www.omicsonline.org/open-access/androgenicanabolic-steroid-boldenone-abuse-as-a-cause-of-dilated-cardiomyopathy-2329-9126.1000153.php?aid=25678 Case Presentation A 34-year old, previously healthy male, presented to the ER with worsening dyspnea over a period of three weeks and the appearance of blood tinged sputum. Soon after presentation, the patient was hypoxemic and required mechanical ventilation. Chest X-ray demonstrated bilateral infiltrates and he was admitted to the ICU with the tentative diagnosis of acute respiratory distress syndrome. Investigation by PICCO, Suggested the presence of heart failure were and the patient was transferred to the ICCU. On admission, the patient maintained normal blood pressure but still needed mechanical support with high FiO2 values to maintain adequate oxygenation. Physical examination was remarkable for his muscular appearance. The heart sounds were regular. The lungs were clear to auscultation, although chest X-ray revealed signs of pulmonary edema. Blood count was remarkable for hemoglobin of 21 gr/dl with hematocrite of 65%. His blood chemistry showed creatinine level on 1.74 mg/dL, with no electrolytes imbalance. LFT were normal, total protein and albumin levels were normal, elevated CK with normal TnT. CRP 10 mg/L (normal level <10 mg/L). Blood cultures and panel of common respiratory infections were all negative. ECG showed normal sinus rhythm, with p pulmonale, signs of hypertrophy and inverted T waves in chest leads. Swan-gantz Cather measurements revealed cardiac output (CO) 3.9, capillary wedge pressure 34 mmHg, SVR 2070 and CI 2.2 consistent with cardiogenic shock. Transthoracic echocardiography demonstrated severe global dysfunction (left ventricular ejection fraction = 20%) with severely dilated left ventricle 5.1 cm (end-systolic diameter), asymmetric hypertrophy (Septum 14 mm, Posterior wall 12 mm). Minimal mitral and tricuspid regurgitation were also noted (Table 1 and Figure 1). During his admission a coronary angiography was preformed, demonstrating normal coronaries arteries. Meticulous repeated history obtained from the patient's family yielded that he had been a kick boxer and a bodybuilder. After asking for all the supplements the patient was taking to be brought to our attention, a vial of Boldenone, an androgenic anabolic steroid (AAS) usually used in veterinary medicine was found. It turned out that the patient was using this illicit drug for his bodybuilding needs. After treating his failing heart, the patient was discharged for outpatient follow-up. During 1 year of follow-up he was treated with a combination of beta-blockers, ACEi and aldactone antagonist according to heart failure guidelines recommendations, with no further admission for either cardiac or non-cardiac causes. Within few months, his cardiac function was partially recovered (EF-40%), also demonstrating improvement in left ventricular chamber measurements and withdrawal of his hypertrophy (Table 1), thus establishing the reversibility of the drug effect Panel A on admission, showing severe LV dysfunction Panel B 1year follow up with improvement of LV function
-
Always aspirate, if you aren't already. Oil (or some other additive) entering the circulatory system could cause flash pulmonary edema/congestive heart failure.
-
This could be a great cruise cycle if your health numbers support it. Some have severe health issues with 100mg test/week (hermatocrit etc), so it is entirely individual. This might be the threshold where you get all the benefits, without the sides. If not, lower accordingly.

